“Hurt people don’t need more isolation.”
- Michael O’Bryan, “Healing from Trauma in the 21st Century”, 4th Annual Social Justice and Cultural Competence, Rowan University (October 2016)
This weekend, I attended Rowan University’s 4th Annual Social Justice and Cultural Competence organized by their Office of Social Justice, Inclusion, and Conflict Resolution. The conference theme was “Communicating Across Differences: Dialogues to Heal Our Communities.” Their keynote presentation resonated with me, so I decided that I would write about it in relation to our class. I was not able to get a hold of a transcript or video for the keynote presentation, so I attached three photos to this post to provide context.
Michael O’Bryan talked about trauma-based care for disadvantaged populations in the 21st Century. He began his presentation with the concept of “militant utopism,” or an imagined world that is both peaceful and strict with issues of equity. O’Bryan presented that most activists will have images of militant utopism in our hearts and aim to move closer to such a reality. O’Bryan also presented that to do so we must consider health beyond the physical to include psychosocial health. We must shift our health practices to ask “what happened to you” instead of “what is wrong with you.”
The following are tips offered to make more inclusive health practices that take into account patients’ history with trauma:
(1) be intentional in the all aspects of your practice, from how you interact with folks on the everyday level to the broader institutional aspects
(2) be compassionate and lower the stakes of risk for all individuals– “keep standards high but expectations low.”
O’Bryan’s presentation relates to our discussion of inherited or generational trauma within groups of people. Throughout the presentation our discussions during the first unit “Historical Antecedents” were in the back of mind, especially in relation to how African American populations feel the effects of slavery and medical disparities presently. His presentation also made me rethink how to engage with social justice to be more compassionate and inclusive. This is something that came up during the conference introduction, my workshop, and the keynote presentation. What baggage do we carry in calling people out on problematic practices? How do we engage with inequitable structures without reproducing a another inequitable structure?
First Photo: Description of the conference
Second Photo: Keynote speaker’s bio
Third Photo: Description of keynote’s talk
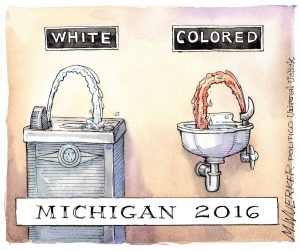 http://usuncut.com/class-war/politico-flint/
http://usuncut.com/class-war/politico-flint/